Blood virology group
Blood virology standards
Biological reference standards are vital to ensure that a measured amount of pathogen – for example Human Immunodeficiency Virus (HIV-1) – in a blood sample is the same from one hospital to another.
Assay sensitivity dramatically improved in the early 1990s with the new polymerase chain reaction (PCR) technology. This allowed laboratories to directly amplify miniscule amounts of genomic material from a pathogen instead of waiting for a detectable antibody response by the host’s immune system.
This led to a rapid development of both commercial and in-house PCR assays, but NIBSC scientists’ early studies showed there was a lack of control material in which to standardise these tests.
In 1995 NIBSC set up an International Working Group on the Standardisation of Genomic Amplification Techniques (SoGAT) to standardise results from one laboratory to another regardless of the assay used. Subsequently NIBSC has produced international standards and secondary working reagents for a range of viruses enabling laboratories and assay manufacturers to calibrate their assay against the same reference standard.
Our group is responsible for developing reference standards for blood-borne viruses and infectious clinical diseases.
International standards:
- are primary ‘gold standards’ in biological reference materials
- are produced with the World Health Organisation (WHO)
- allow direct comparison between different assays and methodologies world-wide
- help standardise the purity, potency and identity measurements for complex biological materials
- have a value assigned in International Units (IU)
- ensure reliability of in-vitro diagnostic procedures used in disease diagnosis and treatment monitoring
They are used to:
- calibrate assays in terms of IU, giving a common unit of reference
- determine assay sensitivity from a standard of fixed concentration
- calibrate secondary working reagents
In a clinical setting it is possible that one laboratory could report a patient sample to contain about 30,000 copies/ml of HIV virus whilst another laboratory could report the same sample to contain nearly 2 million copies/ml. This would have a big impact on patient drug management.
However since the1st International Standard for HIV-1 polymerase chain reaction (PCR) was established 10 years ago, there is much better agreement between the different assays that have been used to measure samples. This is a direct result of the assay manufacturers having a common reference material to use in the development of their assays.
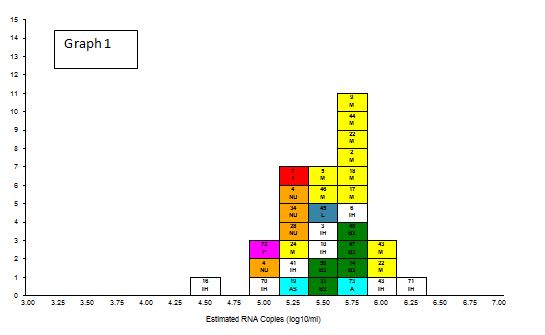
Graph 1 shows the distribution of results from different assays (shown with different coloured blocks) reported during the analysis of material to establish the 1st international standard for HIV-1 RNA. There is nearly a two log variation in results reported by laboratories all testing the same sample.
In a clinical setting it is therefore possible that one laboratory could report the patient sample to contain about 30,000 copies/ml of HIV virus whilst another laboratory could report the same sample to contain nearly 2 million copies/ml! This would have a big impact on patient drug management.
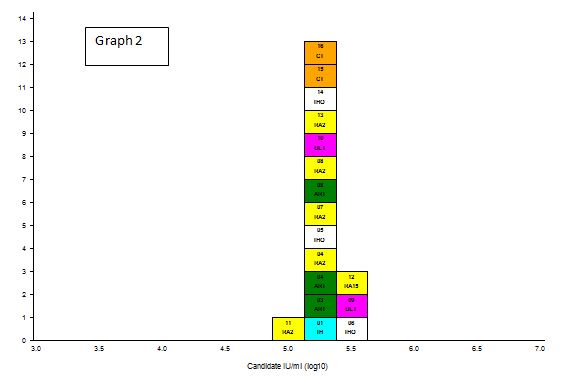
Graph 2 shows the distribution of results from different assays 10 years after the establishment of the 1st International Standard for HIV-1 RNA. Clearly there is much better agreement between the different assays that have been used to measure the sample. This is a direct result of the assay manufacturers having a common reference material to use in the development of their assays.
Secondary working reagents
These are used frequently in assays as daily run controls and indicators of performance.
They monitor the consistency of assay or system performance over time and are calibrated against the primary international standard where possible.
Production complies with the EU in-vitro Diagnostic Device Directive (IVDD) to provide information on patient diagnosis or safety with potential recipients.
Conformance to IVDD is shown by displaying a CE mark.
Regularly including working reagents in a test means laboratories can detect trends. Trends can be attributed to changes in kit batch, operator performance and decline in instrument performance.

NIBSC scientists have developed an online result reporting system for real-time entry of results so that laboratories can monitor data trends.
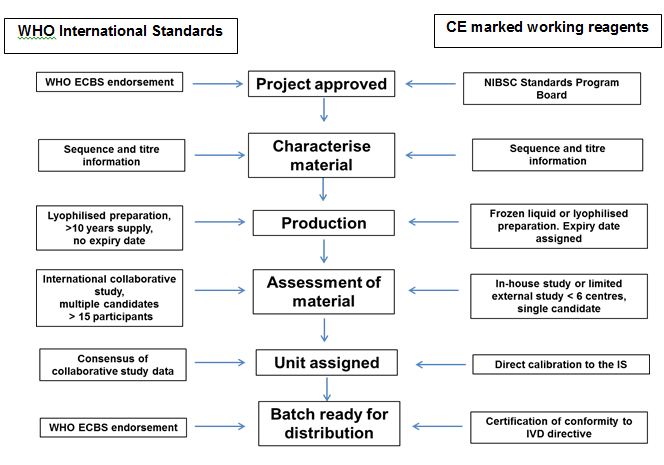
Producing and validating international standards and working reagents involves a number of steps with similarities and differences.
Future developments
The field of clinical diagnostics presents new challenges. Testing is often performed on a range of samples types – such as whole blood, plasma, urine and stools – often with numerous combinations of in-house amplification and detection methods.
In a recent NIBSC study a Norovirus preparation was sent to 25 diagnostic laboratories all using ‘highly sensitive’ in-house assays for the detection of Norovirus GII.
From the data returned it was clear that there was considerable variability with repeat results for the same laboratory as well as from one laboratory to another. In two cases the assay the laboratories were using failed to detect the sample altogether.
International standards and secondary working reagents are now in development for a range of clinical diseases.